
Testimony for the House Ways and Means Hearing, “Pathways to Universal Health Coverage,” Wednesday, June 12, 2019
Thank you for the opportunity to submit testimony to this committee on the pathway to universal health coverage. This is an urgent issue that requires immediate attention in a serious and deliberate manner. I urge you to focus on current legislation, HR 1384, The Medicare for All Act of 2019, sponsored by Congresswoman Pramila Jayapal and co-sponsored by 112 Members of Congress as the best bill that will provide universal coverage and control healthcare spending.
The healthcare crisis in the United States is worsening: infant and maternal mortality rates are high compared to other wealthy nations, the disease burden is great, and over 60 percent of people in the United States delay or forego health care because of the cost, even though most of those surveyed had health insurance.
Life expectancy in the United States has lagged behind other wealthy nations for decades and is now falling farther behind (see the chart below).
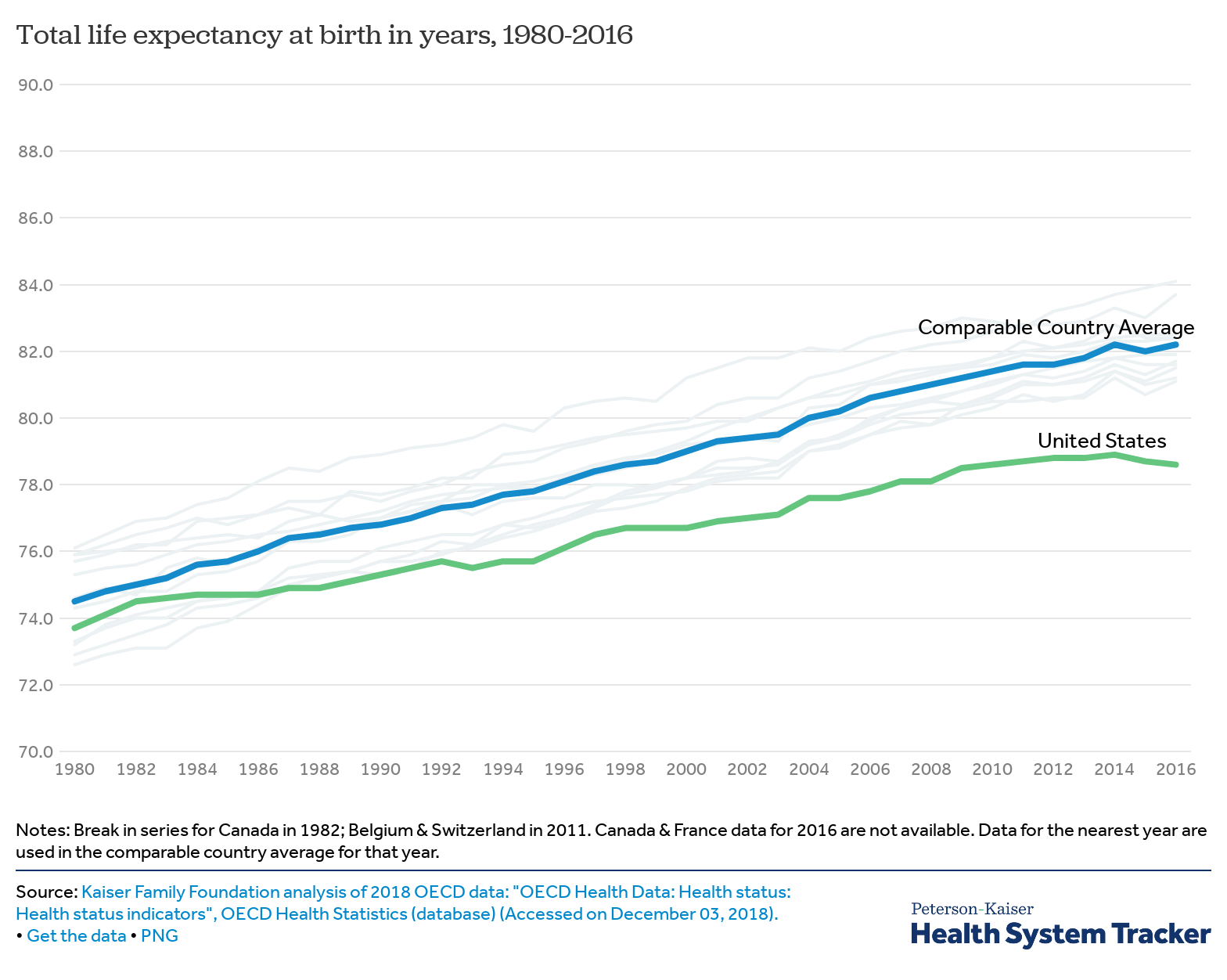
The wealthy countries represented in the chart above all have a universal healthcare system in common, whether it is a mostly socialized system as in the United Kingdom, a Medicare for all system as in Canada or a heavily regulated insurance-based system as in Switzerland.
Another characteristic that other wealthy nations have in common is spending less per capita per year on health care; in some cases, they spend less than half of what the United States spends. The most efficient healthcare systems are either socialized or are similar to original Medicare in the United States.
For decades, healthcare advocates in the United States have promoted a National Improved Medicare for All single payer healthcare system. That system was best exemplified by Congressman John Conyers’ bill HR 676, The Expanded and Improved Medicare for All Act. The closest legislation to that is Congresswoman Pramila Jayapal’s bill HR 1384, The Medicare for All Act of 2019.
Important characteristics of National Improved Medicare for All are:
Universal – All residents are included in the system from birth to death. Universal coverage provides the greatest health security, particularly guarding against epidemics and pandemics. This also creates a single, large risk pool, which reduces the individual burden.
Automatic inclusion – Automatic enrollment simplifies the system and reduces administrative costs. There is no need to determine if someone is eligible or not other than proof of residency.
Comprehensive benefits – Coverage would include all necessary care to guarantee the best health outcomes and so that supplemental insurance is not required. The more insurance plans there are, the more complicated and expensive the system will be.
Nationwide network of providers – All licensed health professionals are in the system so patients can choose where to seek care and are covered no matter where they travel in the United States and its territories. This allows patients to seek treatment at centers that have expertise in their particular ailment without fear of being out of network and having to pay for care out of pocket.
No financial barriers to care – Out-of-pocket costs in the form of co-pays, co-insurance and deductibles create a greater administrative burden and serve as financial barriers that prevent patients from seeking necessary care. The result can be a worsening of disease that becomes more expensive to treat and may have long term consequences.
Single publicly-administered fund – A single public fund to cover healthcare costs is the most efficient. Funds are collected through appropriation of current healthcare dollars, such as those used for Medicare, Medicaid, public employee health benefits and Tricare, and taxes to cover the remainder. The fund is then used to reimburse health professionals, cover infrastructure costs and provide global budgets to health facilities. This would eliminate the need for private health insurance, other than in a complementary role.
Negotiated prices for goods and services – A national health program has the leverage to negotiate fair prices for goods and services. Currently, there is no rational basis for the costs of care resulting in wide disparities in the price of procedures depending on where care is sought and overcharging for goods such as pharmaceuticals.
Global budgets – Every health facility such as a hospital or rehabilitation center would receive a global budget to cover operating expenses and a separate budget for capital investment, which would allow the most effective allocation of resources. An operating budget would allow hospitals to focus on the delivery of care without excessive administrative burden. A separate capital budget would guarantee that new investment is prioritized based on need. A global budget would prevent hospital closures and permit rebuilding health infrastructure in medical deserts.
Rejection of managed care models – Managed care was created decades ago under the assumption that overuse of care was the cause of high healthcare spending. In reality, while a few overuse healthcare services, the majority underutilize services. The high cost of our current healthcare system is due to excessive bureaucracy and prices for goods and services. Managed care incentivizes health professionals to restrict care, which can harm patients, while doing nothing to address bureaucracy and high prices.
Rejection of value-based payment mechanisms – Value-based payments, as included in MACRA, have placed greater financial risk onto health professionals, especially those caring for marginalized populations, and have placed more of an administrative burden onto providers, taking time away from direct patient care. A national health program will permit easy identification of providers who are outliers in terms of the health outcomes of their patients so that remedial steps can be taken.
Adequate workforce – The United States currently lacks adequate numbers of primary care providers, the backbone of high quality healthcare systems. A simplified national health program will draw practitioners away from current administrative positions and return them to direct patient care. The system will also plan and prepare to meet workforce needs to guarantee adequate numbers and distribution of providers.
Just transition – An estimated 3 million people work in administrative jobs related to health care. Under a national health program, the number of people required to handle bureaucracy would be greatly reduced. For those who are displaced from their current job under the new system, they should have priority to be hired into the new system or to receive salary support and training while they transition to new employment. To put this in perspective, 60 million people are separated from their job each year, including 20 million who are fired.
A national health program that has the above features would achieve universal coverage, allow appropriate health planning for the nation and save money. The above system is conservatively estimated to save more than $2 trillion over ten years than if we remain on the present course.
Additional features to consider are:
Universal transition – Other countries that created universal healthcare systems had a planning period of up to eighteen months and then launched the system all at once, including everyone from the start. Considering that the United States is spending enough money at present to provide universal comprehensive coverage and that the greatest savings will be achieved when everyone is in a single, publicly-funded system, it makes the most sense to include everyone at the beginning. We already have a national system for paying providers through the Center for Medicaid and Medicare Services.
Eliminating Investor-owned health facilities – HR 676 had a provision to buy out investor-owned health facilities. There is no reason why a public healthcare system should carry the financial burden of covering investor profits. The cost of buying out all investor-owned health facilities using a 15-year treasury bill at 3 percent is estimated to be $12.75 billion annually, which is about one percent of hospital costs. The facilities could then be kept open as healthcare providers and managed by a public or non-profit entity. The risk of not buying out facilities is that investors may convert them to other profit-making ventures or sell them to developers and those health facilities would be lost.
In summary, I appreciate your interest in finding a path to universal coverage. I urge you to take advantage of the decades of work done by single payer healthcare advocates and the current legislation introduced by Congresswoman Jayapal, HR 1384.
Single payer healthcare, also called National Improved Medicare for All, is widely supported by the public and by health professionals. Recent polls indicate 70 percent support.
The time for debate about what type of healthcare system we need is over. The public has chosen National Improved Medicare for All. Let’s begin the process of making HR 1384 a reality. I urge the Committee to hold substantive hearings that include experts who can testify on the merits of HR 1384 and answer committee members’ questions. There are numerous institutions and people in the United States who have this expertise. I look forward to working with you on this.
Margaret Flowers, M.D.
National coordinator, Health Over Profit for Everyone (HOPE)


